

An alpha thalassemia gene mutation reduces or stops alpha-globin production by altering or deleting the HBA1 and HBA2 genes on chromosome 16, disrupting hemoglobin balance and causing anemia ranging from silent to severe.
Alpha thalassemia ranks among the most common inherited blood disorders on the planet, affecting millions of carriers across Southeast Asia, the Mediterranean, the Middle East, and parts of Africa. Most carriers never know they have it—until a routine blood test, a puzzling anemia diagnosis, or a family planning conversation brings it to light.
At the root of every case sits a small, precise set of genetic instructions gone wrong. An alpha thalassemia gene mutation interferes with how the body builds alpha-globin chains, the protein components hemoglobin needs to carry oxygen. The difference between a healthy carrier and a child facing life-threatening anemia often comes down to a single deleted gene.
This guide breaks the genetics down in plain language. You’ll learn how the HBA1 and HBA2 gene mutations affect hemoglobin, how alpha globin gene deletion drives most cases, why chromosome 16 alpha thalassemia is so common, and what the latest diagnosis and treatment options offer. Whether you’re a student, a healthcare professional, or someone navigating a family history of anemia, this is your foundation for understanding the condition.
What Is an Alpha Thalassemia Gene Mutation?
 An alpha thalassemia gene mutation is any genetic change—deletion or point mutation—that reduces or eliminates the production of alpha-globin chains. These chains are essential building blocks of hemoglobin, the protein inside red blood cells that carries oxygen from your lungs to every tissue in your body.
An alpha thalassemia gene mutation is any genetic change—deletion or point mutation—that reduces or eliminates the production of alpha-globin chains. These chains are essential building blocks of hemoglobin, the protein inside red blood cells that carries oxygen from your lungs to every tissue in your body.
Healthy adult hemoglobin, called Hemoglobin A (HbA), is made of four protein chains: two alpha-globin chains and two beta-globin chains. This balanced structure keeps red blood cells stable and oxygen flowing efficiently. HbA makes up over 95% of the hemoglobin in adults. When an alpha thalassemia gene mutation disrupts alpha-chain production, this balance collapses and leads to the clinical features of the disease.
Why Is Alpha Thalassemia So Common Worldwide?
Alpha thalassemia is one of the most widespread genetic conditions on Earth, with especially high carrier rates in regions where malaria was historically common. Carriers of certain alpha-globin gene deletions gained a survival advantage in malaria-prone areas, which helped these traits persist across generations. According to the World Health Organization, expanded screening and genetic counseling can significantly reduce the number of children born with severe forms.
The Role of HBA1 and HBA2 Genes
Two genes are responsible for producing alpha-globin chains: HBA1 and HBA2. Both genes live on chromosome 16, sit very close to one another, and produce identical alpha-globin proteins. Most people inherit four functional alpha-globin genes—two from each parent—giving the body the steady supply of alpha chains it needs.
What Is the Structure and Function of the Alpha-Globin Genes?
The HBA1 and HBA2 genes activate during red blood cell formation in the bone marrow. They direct the synthesis of alpha-globin chains, which combine with beta-globin chains to form stable Hemoglobin A. The finished hemoglobin then transports oxygen through the bloodstream.
Because both genes produce identical proteins, the total count of working genes matters more than which specific gene is affected. When all four genes work correctly, hemoglobin stays stable, circulation runs smoothly, and energy levels remain normal. You can explore each gene’s contribution in our detailed guide on HBA1 and HBA2 gene function.
How Do HBA1 and HBA2 Gene Mutations Affect Hemoglobin Production?
HBA1 and HBA2 gene mutations reduce or eliminate alpha-globin chain production. When alpha chains fall short, beta chains in adults (or gamma chains in fetuses) are left without partners. These leftover chains clump together into unstable structures that damage red blood cell membranes, leading to premature cell destruction and chronic anemia.
This concept, known as gene dosage, is central to the disease. The more genes affected by an alpha thalassemia gene mutation, the less alpha-globin the body produces—and the more severe the resulting anemia becomes. This dose-dependent relationship explains why the condition ranges from a silent carrier state to a fatal form.
Mechanisms of Alpha Globin Gene Deletion
 Most cases of alpha thalassemia trace back to alpha globin gene deletion—the physical loss of one or more alpha-globin genes from chromosome 16. A smaller share comes from non-deletional point mutations, where the gene stays present but stops working properly.
Most cases of alpha thalassemia trace back to alpha globin gene deletion—the physical loss of one or more alpha-globin genes from chromosome 16. A smaller share comes from non-deletional point mutations, where the gene stays present but stops working properly.
What Are the Common Deletion Patterns?
Doctors classify alpha globin gene deletion by the specific DNA segments lost:
- Single-gene deletions (-α3.7 and -α4.2): These remove one alpha gene and leave one functional gene on the affected chromosome. They are the most common deletions seen worldwide.
- Double-gene deletions (–SEA and –MED): The Southeast Asian (–SEA) and Mediterranean (–MED) deletions remove both HBA1 and HBA2 from a single chromosome, leading to more serious clinical outcomes.
Most deletions occur through non-allelic homologous recombination (NAHR) during meiosis—the cell division that creates eggs and sperm. The alpha-globin gene cluster contains repetitive DNA sequences known as Z boxes and X boxes. Because these repeats look so similar, chromosomes can misalign during pairing. When misaligned chromosomes swap genetic material, one ends up with a deletion and the other with a duplication. The chromosome carrying the deletion passes the alpha thalassemia gene mutation to the next generation. Our breakdown of the alpha globin gene deletion mechanism explains exactly how chromosomes misalign.
What Less Common Patterns Have an Impact?
While unequal crossing over explains most cases, rarer events also occur. Larger gross deletions can remove regulatory regions that control alpha-globin genes, even when the genes themselves stay intact. Non-deletional mutations include point mutations, splice site mutations, promoter and regulatory region changes, and frameshift mutations. Unlike full deletions, these often allow partial alpha-globin production, so disease severity can vary widely depending on the mutation type and combination.
Chromosome 16 and Alpha Thalassemia
Chromosome 16 sits at the center of this disorder. Understanding its structure explains why alpha thalassemia gene mutations are so frequent.
Where Are the Alpha-Globin Genes Located on Chromosome 16?
The alpha-globin gene cluster sits on the short arm of chromosome 16, near the telomere at position 16p13.3. This region is highly active during genetic recombination, which is exactly why it becomes a hotspot for deletions. HBA1 and HBA2 share nearly identical DNA sequences—a feature that supports steady alpha-globin production but carries a hidden risk.
What Are the Implications of Chromosome 16 Alpha Thalassemia Abnormalities?
Because the two genes look so alike, chromosomes can misalign during cell division. This misalignment sets the stage for the deletions and duplications behind chromosome 16 alpha thalassemia. The location and structure of this region directly shape inheritance patterns, which is why molecular testing—not just a blood count—is essential for at-risk couples planning a family.
Types and Severity of Alpha Thalassemia
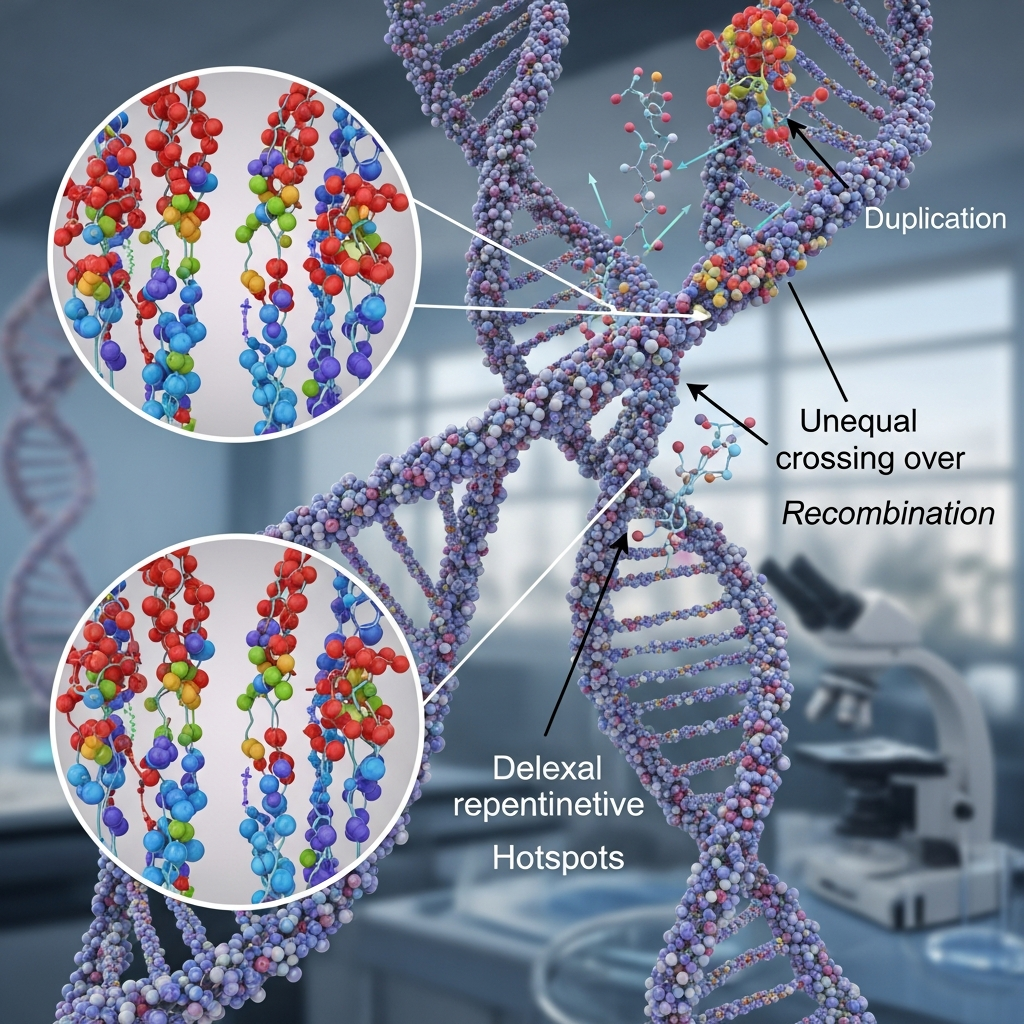
 One of the most predictable patterns in all of genetic medicine is the relationship between the number of affected alpha-globin genes and disease severity. The gene count maps directly onto the clinical picture.
One of the most predictable patterns in all of genetic medicine is the relationship between the number of affected alpha-globin genes and disease severity. The gene count maps directly onto the clinical picture.
Silent Carrier State
When one of four genes is affected (-α/αα), the result is a silent carrier. These individuals have normal hemoglobin, no symptoms, and the condition is usually found only through genetic screening.
Alpha Thalassemia Trait (Minor)
When two genes are affected, the result is alpha thalassemia trait—mild microcytic anemia with small red blood cells, often mistaken for iron deficiency. Our complete guide to the alpha thalassemia trait covers testing and care in detail.
Hemoglobin H Disease
When three genes are affected, the result is Hemoglobin H disease. The severe shortage of alpha chains lets excess beta chains form unstable Hemoglobin H. Patients face moderate to severe hemolytic anemia, an enlarged spleen, and sometimes bone changes.
Hydrops Fetalis (Major)
When all four genes are affected, the result is Hemoglobin Bart’s hydrops fetalis—the most severe form. With no alpha-globin at all, the fetus produces Hemoglobin Bart’s, leading to massive fluid buildup and heart failure. This condition is usually fatal before or shortly after birth.
How Is an Alpha Thalassemia Gene Mutation Diagnosed?
Standard blood tests can hint at alpha thalassemia, but they rarely confirm it. Diagnosis usually follows a layered approach that moves from indirect clues to direct genetic evidence.
What Genetic Testing Methods Are Used?
- Complete Blood Count (CBC): Often reveals microcytosis—red blood cells smaller than normal—and reduced MCH.
- Hemoglobin electrophoresis or HPLC: May detect abnormal hemoglobins like Hb H or Hemoglobin Bart’s, though results are often normal in milder cases.
- Gap-PCR: A fast, commonly used method that identifies frequent deletions.
- MLPA (Multiplex Ligation-dependent Probe Amplification): Maps deletions across the alpha-globin gene cluster with high accuracy.
- Next-Generation Sequencing (NGS): Identifies rare deletions, non-deletional mutations, and complex rearrangements missed by older tests.
Genetic testing is considered the gold standard because it identifies the underlying cause directly. Choose molecular testing if confirming carrier status matters more to you than a quick preliminary screen—especially when both partners may carry deletions.
How Do Prenatal Diagnosis and Newborn Screening Work?
Prenatal diagnosis uses chorionic villus sampling or amniocentesis to analyze fetal DNA, allowing at-risk couples to learn whether a pregnancy is affected by a severe form. Newborn screening programs in many regions test for abnormal hemoglobins shortly after birth, catching cases early so families can begin monitoring and care. Accurate, early diagnosis also prevents unnecessary iron supplementation in carriers whose anemia is genetic, not iron-related.
Management and Treatment Options
 Treatment depends entirely on severity, which the deletion count predicts. There is no one-size-fits-all approach—care is tailored to the individual.
Treatment depends entirely on severity, which the deletion count predicts. There is no one-size-fits-all approach—care is tailored to the individual.
Symptomatic Treatment for Hemoglobin H Disease
Silent carriers and those with the trait need no treatment, though they should avoid unnecessary iron supplements. Hemoglobin H disease care often includes folic acid supplementation, periodic blood transfusions during anemic crises, and sometimes splenectomy to extend the lifespan of red blood cells.
Blood Transfusions and Chelation Therapy
Severe cases may require regular blood transfusions to maintain healthy hemoglobin levels. Because repeated transfusions can cause iron overload, chelation therapy is used to remove excess iron and protect organs like the heart and liver from long-term damage.
Bone Marrow Transplantation
For the most severe cases, bone marrow or stem cell transplant offers a potential cure. A successful transplant replaces the patient’s faulty blood-forming cells with healthy donor cells, though the procedure carries significant risks and requires a closely matched donor.
Gene Therapy: Future Prospects
Gene therapy offers the most promising path forward. Researchers are developing techniques to harvest a patient’s own hematopoietic stem cells, insert functional alpha-globin genes, and transplant them back—potentially curing the condition without lifelong transfusions. Gene-editing tools like CRISPR may expand these possibilities even further.
Genetic Counseling and Family Planning
Because alpha thalassemia is inherited, understanding your genetic status before starting a family carries real weight.
Why Does Carrier Screening Matter?
Couples who are both carriers face a higher chance of having a child with a severe form. When a parent carries a double-gene deletion like –SEA, two carrier partners can produce a child with hydrops fetalis. Carrier screening identifies this risk early, giving families the widest range of choices and the most time to plan.
What Reproductive Options Do Affected Couples Have?
Affected couples can pursue several paths, including prenatal diagnosis with the option to prepare for a severe outcome, and IVF with preimplantation genetic testing, which screens embryos before implantation. Our family planning thalassemia guide covers carrier screening, prenatal diagnosis, and these reproductive choices in detail.
Living With Alpha Thalassemia
For most people with the trait or silent carrier status, life carries on as normal. Those with Hemoglobin H disease may need some adjustments.
What Lifestyle Adjustments Help?
People with Hemoglobin H disease benefit from regular medical monitoring, folic acid supplementation, and avoiding iron supplements unless prescribed. Staying alert to infections—which can trigger anemic crises—and maintaining a balanced diet support overall blood health. Avoiding certain oxidizing medications, as advised by a hematologist, helps protect fragile red blood cells.
Where Can You Find Support Networks and Resources?
Patient advocacy groups, online communities, and thalassemia foundations offer emotional support, practical advice, and up-to-date information. Connecting with others who share the diagnosis can ease the isolation that often comes with a rare condition.
Research and Future Directions
 The future of alpha thalassemia care is moving fast, driven by advances in genetics and biotechnology.
The future of alpha thalassemia care is moving fast, driven by advances in genetics and biotechnology.
How Are Advances in Gene Editing Reshaping Treatment?
CRISPR and other gene-editing tools may soon allow doctors to correct alpha thalassemia gene mutations directly within a patient’s stem cells. Early-stage research aims to restore normal alpha-globin production, offering hope for a one-time cure rather than lifelong management.
What New Therapeutic Targets Are Emerging?
Researchers are exploring drugs that reduce globin chain imbalance, agents that improve red blood cell survival, and Next-Generation Sequencing to tailor treatment to each patient’s exact genetic profile. These targeted approaches could transform care for those with more severe forms.
Conclusion
An alpha thalassemia gene mutation comes down to a few core ideas. The HBA1 and HBA2 genes on chromosome 16 produce the alpha-globin chains that hemoglobin needs. When deletions or point mutations strike these genes, alpha-globin production drops, the alpha-to-beta chain balance collapses, and unstable hemoglobin forms. The number of affected genes predicts severity with remarkable precision—from silent carriers to fatal hydrops fetalis.
If you or your partner has a family history of anemia, the most valuable next step is simple: consult a hematologist or genetic counselor about comprehensive genetic screening. Early knowledge gives families the widest range of choices and the most time to plan. The Centers for Disease Control and Prevention and the World Health Organization offer trusted guidance on screening and care.
Frequently Asked Questions
1. What is an alpha thalassemia gene mutation?
An alpha thalassemia gene mutation is a genetic change—either a deletion or a point mutation—in the HBA1 or HBA2 genes on chromosome 16. It reduces or stops alpha-globin production, disrupts hemoglobin balance, and causes anemia that ranges from silent to severe.
2. How do HBA1 and HBA2 gene mutations differ?
HBA1 and HBA2 produce identical alpha-globin proteins, so the total number of working genes matters more than which one is affected. A mutation in either gene reduces alpha-globin supply, but the effects grow more serious when both genes are affected at the same time.
3. Can alpha thalassemia be cured?
Most forms cannot be cured today, though symptoms can be managed with monitoring, transfusions, and folic acid. Severe cases may be treated with bone marrow or stem cell transplant, and experimental gene therapy shows strong future promise.
4. What are the symptoms of alpha thalassemia?
Symptoms range from none in silent carriers to mild anemia in the trait, and moderate to severe anemia, fatigue, and an enlarged spleen in Hemoglobin H disease. The most severe form, hydrops fetalis, is usually fatal before or shortly after birth.
5. How is alpha thalassemia inherited?
Alpha thalassemia follows an autosomal recessive pattern. A child must inherit affected genes from both parents to develop a severe form, which is why carrier screening matters so much for couples planning a family.
6. What is the difference between alpha thalassemia minor and major?
Alpha thalassemia minor (the trait) involves two affected genes and causes only mild anemia. Alpha thalassemia major refers to the most severe form, Hemoglobin Bart’s hydrops fetalis, where all four genes are affected, and the condition is usually fatal before or shortly after birth.
7. Is genetic counseling recommended for alpha thalassemia carriers?
Yes. Genetic counseling helps carriers understand their inheritance risk, especially when both partners may carry deletions. It gives couples the information they need to make informed reproductive decisions and reduces the chance of a child being born with a severe form.
8. What is the role of chromosome 16 in alpha thalassemia?
Chromosome 16 carries the HBA1 and HBA2 genes at position 16p13.3. The repetitive, nearly identical DNA sequences in this region make chromosomes prone to misalignment during cell division, which is why chromosome 16 alpha thalassemia deletions are so common.
9. Are there any new treatments for alpha thalassemia?
Yes. Gene therapy is the most promising advance, aiming to insert functional alpha-globin genes into a patient’s own stem cells. Gene-editing tools like CRISPR and improved molecular diagnostics are also expanding treatment options for severe cases.
10. How does alpha globin gene deletion impact health?
Alpha globin gene deletion reduces the supply of alpha-globin chains, disrupting hemoglobin balance. The more genes deleted, the more severe the anemia—ranging from no symptoms with one deletion to life-threatening disease when all four are lost.








{kind=link}